Cpt Code For Thromboendarterectomy With Patch Graft
A PTE has significant risk; mortality for the operation is typically 5%, but less in centers with high volume and experience. Individuals with favorable hemodynamic risk profiles also demonstrate lower mortality rates (1.3%). PTEs are risky because of the nature of the procedure. PTEs involve a full (CPB), deep and cardioplegia (a crystalline fluid which stops the heart from beating). Actual removal of the embolus carried out in a (deep hypothermia and periods of cessation of circulation). There are a number of reasons why these high risk elements of the procedure are necessary.
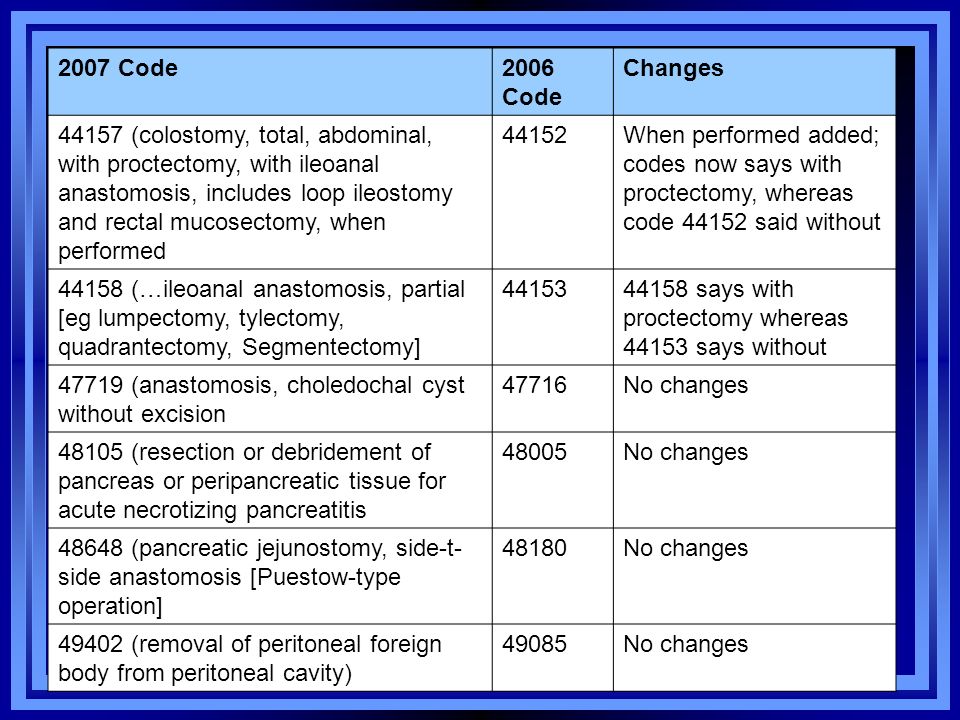
Anesthesia for procedures on arteries of knee and popliteal area; popliteal thromboendarterectomy, with or without patch graft 01444 Anesthesia for procedures on arteries of knee and popliteal area; popliteal excision and graft or repair for occlusion or aneurysm.
CPB is needed to divert blood from the heart and lungs and supply the body with oxygen and blood while the pulmonary vasculature is operated on. Cardioplegia is initiated as the approach to the pulmonary arteries is performed through the pericardium, a fibrous sack surrounding the heart. Furthermore, movement from the heart makes delicate work on the closely attached pulmonary arteries complex. Hypothermia is necessary as the embolus is very delicate and the risk of disruption is high, in order to appropriately visualize the clot and remove it a bloodless field is required. Cara mengatasi windows activation key. Clot visualization is achieved through dissection of the pulmonary arteries which is technically challenging. If possible the clot is removed in a single piece to avoid the formation of mobile emboli. In order to achieve this CPB is periodically stopped, resulting in a complete cessation of blood circulation.
This is only feasible if the patient is hypothermic (cooled to 18-20C) as metabolism is slowed and the body can better tolerate the resulting lack of blood supply. Circulatory arrest is limited to 20 minute intervals to protect brain function. Typically an experienced surgeon can perform an entire unilateral procedure in this time.
After each interval of arrest circulation is continued for 10 minutes or until pulmonary venous oxygen saturation is at least 90%. Bypass time is typically 345 minutes. There are emerging alternative options available that seek to limit neurologic complications resulting from hypothermia and circulatory arrest. Currently these options have not been shown to be superior to the previously described technique.
 Dubbing mixer. Property master (as Dave Procter). Production buyer Sound Department.
Dubbing mixer. Property master (as Dave Procter). Production buyer Sound Department.
They include use of moderate hypothermia, antegrade cerebral artery profusion without total circulatory arrest, and negative pressure application to the left ventricle. It is important to note that acute is a dramatically different procedure. Its is typically performed without hypothermia as the structure of the clot is different, and the emergent nature presents different operative priorities.

Recovery and Complications. Recovery from this procedure can be complex. Thoracic surgery, CBP and cardioplegia are associated with their own complications and management challenges, as is hypothermia.